What Happens If Telehealth Abortion Is Restricted Nationally?
Telehealth abortion has quietly transformed reproductive healthcare in America. For millions of people particularly those in rural communities, lower-income households, and states with shrinking clinic access it hasn’t just been a convenient option. It’s been the only realistic one.
Now that access is under real and growing threat, the questions people are asking have shifted from “how do I use telehealth abortion?” to something more urgent: what happens if it goes away?
This guide cuts through the speculation. Here’s what a nationwide telehealth abortion restriction would actually mean, who it would hurt most, what options would remain, and most importantly what you can do right now while full protections are still in place.
What Does “Nationwide Telehealth Abortion Restriction” Actually Mean?
Before anything else, it’s worth being precise about what “restriction” means because this word is doing a lot of work in a lot of different conversations, and conflating different types of restrictions leads to both unnecessary panic and dangerous complacency.
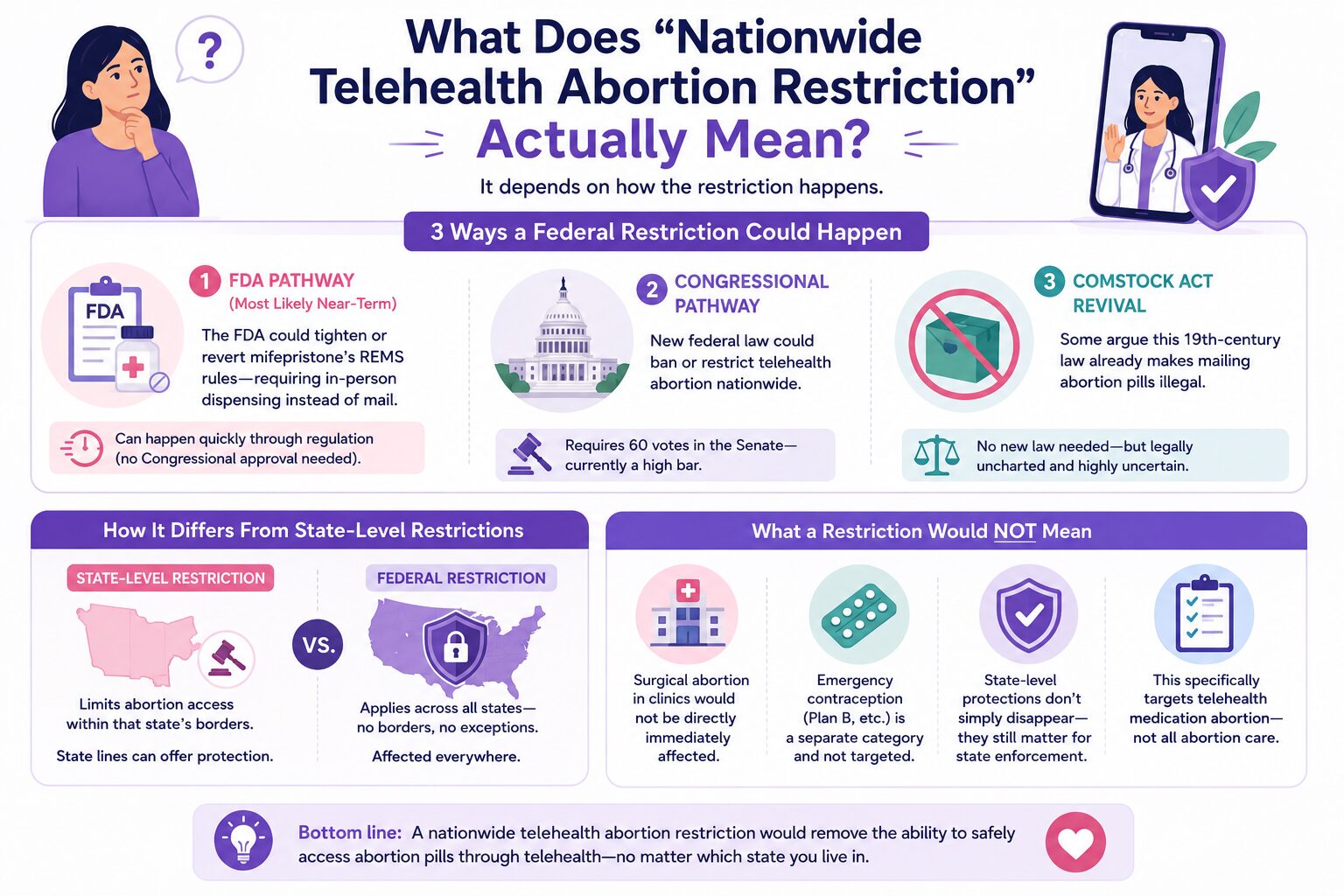
A state-level restriction means abortion access is limited within that state’s borders. Many states already have these. But people in protected states like Illinois, California, or New York have largely been insulated from those restrictions, able to access telehealth care from home, legally and safely.
A federal restriction is categorically different. It would not respect state lines. It would not be blocked by shield laws in the way out-of-state prosecutions can be. It would reach into currently protected states and change the landscape for everyone, not just those already living under restriction.
There are three distinct pathways a federal restriction could take, and they matter because each has a different timeline and a different set of workarounds:
The FDA pathway is currently the most likely near-term mechanism. The FDA controls the mifepristone REMS (Risk Evaluation and Mitigation Strategy) program. Before 2021, mifepristone could only be dispensed in-person at certified clinics not mailed to patients. Reverting or tightening those REMS requirements doesn’t require Congressional approval. It can happen through regulatory action alone, which makes it faster and less predictable than legislation.
The Congressional pathway would require legislation and currently, that means clearing a 60-vote Senate threshold. That’s a high bar given the current political landscape, which makes full congressional action less likely in the near term but not impossible over a longer horizon.
The Comstock Act revival is perhaps the least understood threat. This is a 19th-century federal law that prohibits mailing “obscene” materials. Some legal advocates are pushing to apply it to abortion pills arguing it already makes mailing mifepristone and misoprostol illegal, without any new legislation needed. Most legal scholars consider this application a significant stretch, but the Supreme Court has not definitively ruled it out.
It’s also important to be clear about what restriction would not mean. Surgical abortion in clinics would not be directly and immediately affected by a telehealth-specific restriction. Emergency contraception like Plan B is a separate category and would not be directly targeted by most proposed restrictions. And state-level protections don’t simply evaporate; they continue to matter for state-level enforcement, even if they can’t shield against federal action.
Who Would Be Hurt Most
Policy analysis becomes real when you understand who actually bears the consequences. And on this issue, the impact would not be evenly distributed.
People in rural and healthcare desert areas are the most immediately vulnerable. For someone living hours from the nearest abortion clinic which describes a significant portion of the American population, telehealth isn’t a preference. It’s the only option that doesn’t require taking days off work, arranging childcare, and covering travel and lodging costs on top of the procedure itself. The clinic access crisis that existed before Dobbs has only deepened since. Telehealth has been filling a gap that physical infrastructure cannot.
If you currently have access, scheduling a telehealth abortion care consultation while full protections are in place is the most direct step you can take right now.
Low-income women face compounding barriers that wealthier patients don’t. Traveling for abortion care means time off work, childcare, transportation, and potentially overnight stays. Abortion funds exist specifically to help cover these costs and they do important work but they are chronically underfunded and simply cannot meet full demand if telehealth is eliminated.
Women in currently protected states are perhaps the least prepared for what federal restriction would mean. Someone in Illinois or New York who has assumed their access is secure may be blindsided by federal action in a way that someone in a state that has been navigating restrictions for years is not. The Illinois Reproductive Health Act provides strong state-level protections but understanding the distinction between state protection and federal exposure matters now more than ever.
Minors, survivors of abuse, and people in unsafe situations rely on telehealth’s unique ability to provide private, home-based care. For someone in an abusive relationship where travel is monitored, or a minor who cannot safely involve a parent, telehealth is not just more convenient, it’s meaningfully safer. Removing that option is not a neutral policy change.
What Would Actually Happen to Medication Abortion Access
Mifepristone is the primary target of most federal restriction efforts and understanding why helps clarify what’s actually at stake.
The FDA’s REMS program for mifepristone has been used as a restriction mechanism before. Prior to 2021, the REMS required in-person dispensing at certified facilities meaning telehealth prescriptions that get mailed to patients weren’t possible. A return to those requirements, or something similar, is the most realistic near-term federal action. It would not ban mifepristone outright, but it would effectively eliminate the telehealth pathway that most people now use.
If you’re currently considering medication abortion, understanding exactly how the abortion pill works, what the process involves, what to expect, and how it’s accessed through a licensed provider is worth doing now, while that access remains fully protected.
Misoprostol is a different story. Because it’s used for other medical purposes, ulcer treatment, labor induction, it doesn’t have abortion-specific prescribing restrictions and is far harder to target directly. The WHO-approved misoprostol-only protocol is increasingly used in contexts where mifepristone is restricted, and understanding what to expect from misoprostol is worth knowing regardless of what policy changes occur.
Mail-order abortion pills represent one of the most direct targets of federal restriction. The Comstock Act argument, if ever accepted by a court, would specifically criminalize the mailing of abortion medication, not necessarily the medication itself. This is why mail-order restriction is often where federal action begins, rather than an outright ban.
As for surgical abortion absorbing the demand if medication abortion is restricted it simply cannot. Clinic capacity has contracted significantly since Dobbs. Surgical abortion waitlists in even relatively accessible states would be overwhelmed if the roughly half of all US abortions currently obtained via medication were suddenly redirected to in-clinic care.
What Options Would Still Exist Under Restriction
This is where fear becomes preparation. Even under significant restriction, options would remain though they would be harder, more expensive, and less private than what currently exists.
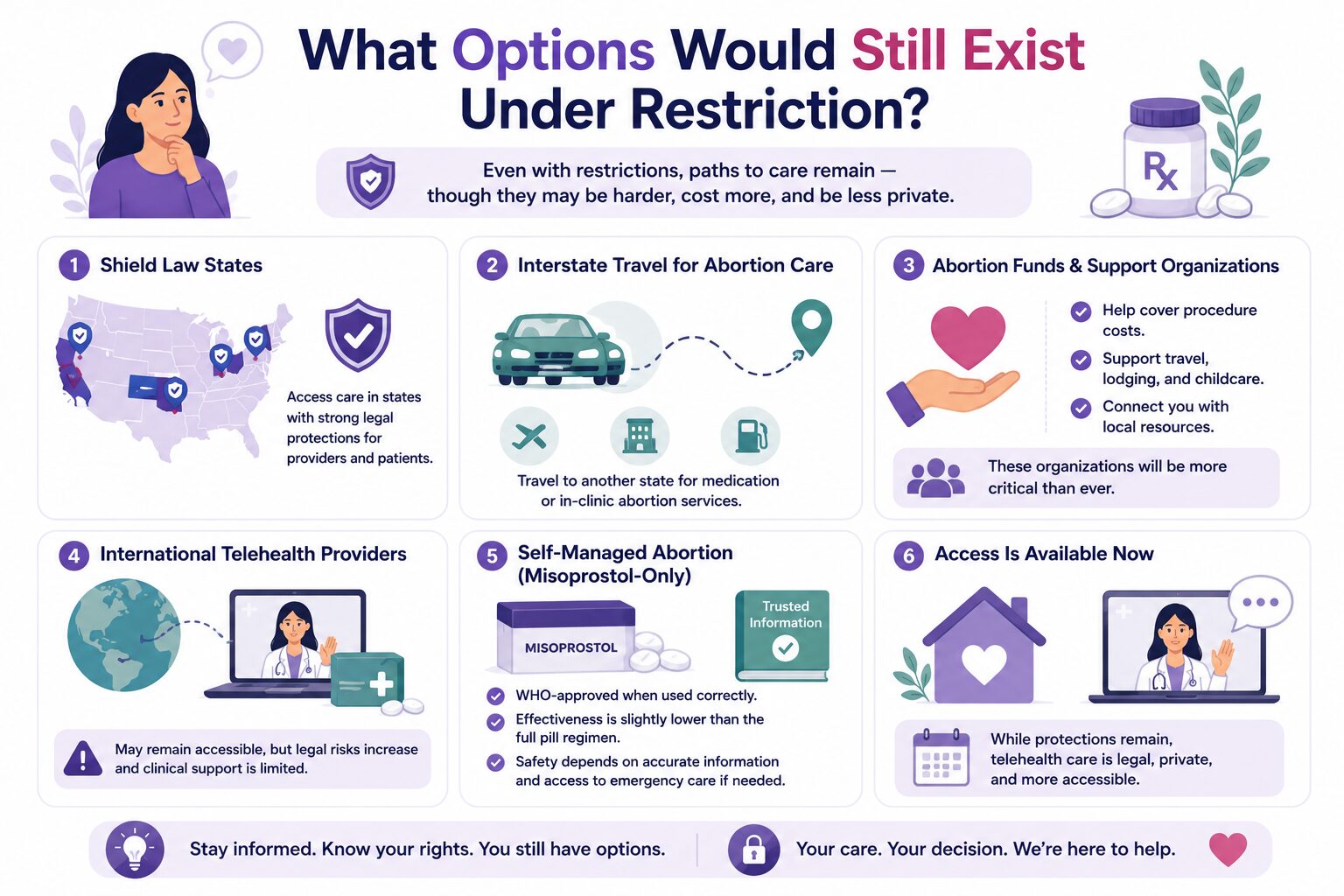
Shield law states like Illinois, California, Colorado, and New York protect providers from out-of-state prosecution. Right now, that protection is robust and meaningful. Under federal action, shield laws cannot protect against federal prosecution but they remain valuable for state-level enforcement contexts. Understanding how abortion shield laws work gives you a clearer picture of what these protections actually cover and what they don’t.
Telehealth abortion care remains one of the most private, accessible, and clinically supported options currently available in protected states. If you’re in a position to access care now, our telehealth abortion care service connects you with licensed clinicians who prioritize your privacy, your safety, and your specific situation without requiring travel or in-person visits. This is the option most at risk under federal restriction, which is precisely why accessing it while full protections exist is the most protected path forward.
In-clinic abortion services would not be directly eliminated by a telehealth-specific restriction and would remain available in states where abortion is legal. For those who prefer or require an in-person option, or whose gestational age makes medication abortion less appropriate, in-clinic abortion services provide a supervised, clinically supported alternative. Under significant restriction, in-clinic capacity would face increased demand, another reason that acting sooner rather than later matters.
Interstate travel for abortion care remains federally protected; the Supreme Court has not restricted the right to travel across state lines for legal medical care. For people in restricted states, traveling to a shield law state for either medication or surgical abortion would remain an option. Traveling for an abortion requires planning, understanding which states to go to, how to cover costs, and what logistics are involved.
Abortion funds and support organizations would become critical infrastructure under restriction. These organizations help cover procedure costs, travel, lodging, and childcare for people who cannot afford to pay out of pocket. Finding abortion financial aid programs in your area before you need them not after is a practical preparation step worth taking now.
International telehealth providers like Aid Access operate outside US jurisdiction and would remain technically accessible in some restriction scenarios. However, the legal risk profile of using international providers increases significantly under heightened federal enforcement, and they operate without the clinical support infrastructure of domestic licensed providers. They represent a safety net, not a first choice.
Self-managed abortion using misoprostol-only protocols increases under restriction historically and predictably regardless of its legal status. The WHO considers misoprostol-only protocols safe and effective when used correctly. The legal risk of self-managed abortion varies dramatically by state, and the medical safety depends heavily on having accurate information and access to emergency care if needed. If you’re in a situation where this feels like your only option, speaking with a provider first even briefly can make a meaningful difference in safety outcomes.
Access is available now. While full telehealth protections are in place, confidential consultations with licensed providers are accessible, private, and legal. Learn whether telehealth abortion is right for your situation before that window narrows.
Digital Privacy Under Restriction
Privacy risks that feel manageable today become significantly more serious under heightened federal enforcement and this is one of the dimensions people are least prepared for.
Search history, location data, and period tracking app data have already appeared in abortion-related legal cases. Under restriction, the investigative interest in this kind of data would only increase. The difference between current privacy risk and risk under active federal enforcement is not incremental, it’s categorical.
Some practical steps that matter now and would matter even more under restriction:
Using private or incognito browsing for abortion-related research prevents local search history from being saved, though it doesn’t protect against your ISP or device-level tracking. A VPN adds a meaningful additional layer. Period tracking apps that store data on company servers are not HIPAA-covered; their data can be subpoenaed, sold, or accessed in ways that your medical records cannot. Encrypted communication with providers protects the content of your conversations in ways that standard email and text messaging do not.
Your medical records held by licensed providers are HIPAA-protected. Your Google searches, your location history, and your period app entries are not. Understanding that distinction is foundational to protecting yourself. Our full abortion privacy guide and online privacy and abortion access resources walk through specific, actionable steps for reducing your digital exposure.
What You Can Do Right Now
The most important thing this guide can tell you is that acting before restrictions take effect is categorically easier and safer than navigating care after they do.
Access care now if you need it. Current telehealth protections in shield law states are more robust than they may be in six to twelve months. Acting while those protections are fully intact means maximum legal protection, no travel required, and full access to licensed clinical support.
Know your state’s current legal landscape. The difference between living in a shield law state and a restricted state has real, practical implications for what you can safely access and how. Illinois residents currently benefit from some of the strongest reproductive privacy protections in the country but knowing specifically what those protections cover puts you in a position to use them effectively.
Identify financial resources before you need them. Abortion funds take time to connect with and often have limited capacity. Knowing what abortion costs and what financial assistance is available before you’re in a time-sensitive situation gives you options you won’t have if you’re starting from scratch under pressure.
Build good digital privacy habits now. The steps that protect your privacy today are the same ones that would protect you under restriction; they’re just easier to implement before urgency is involved.
Stay informed through reliable sources. The Guttmacher Institute, ACOG, and Plan C are among the most reliable sources for policy updates on medication abortion access. Reproductive healthcare journalism at established outlets is more reliable than social media for legal developments and on this topic, the stakes of misinformation are too high to rely on viral content.
Have questions about your specific situation? Explore your options with clinician-reviewed information tailored to where you are and what you need.
Frequently Asked Questions
Can the federal government actually ban telehealth abortion nationwide?
Yes, through multiple pathways. The FDA can modify the mifepristone REMS program to require in-person dispensing without Congressional approval, which makes it the most likely near-term mechanism. Congress could also pass legislation, though clearing a 60-vote Senate threshold is currently difficult. Executive enforcement directives represent a third pathway. None of these require a single sweeping “ban” incremental restriction through regulatory change is the more realistic scenario.
Would a federal restriction override Illinois’s shield law protections?
Shield laws protect providers from prosecution by other states; they are effective against interstate enforcement actions. However, they generally cannot override federal law under the Constitution’s Supremacy Clause. Federal action would reach into shield law states in ways that out-of-state prosecution cannot. This is why people in Illinois and other currently protected states should not assume their access is indefinitely secure under federal action.
What would happen to abortion pills specifically if telehealth is restricted?
The most likely scenario involves tightening the mifepristone REMS to require in-person dispensing again, effectively ending mail-order access for that medication without banning it outright. Misoprostol is harder to restrict because it has multiple non-abortion medical uses. A misoprostol-only protocol, while less effective than the combination regimen, would remain more accessible than mifepristone under tightened REMS.
Would surgical abortion still be available if telehealth abortion is restricted?
Surgical abortion in clinics would not be directly affected by a telehealth-specific restriction. However, existing clinic capacity cannot absorb the full demand that medication abortion currently serves. Since Dobbs, clinic closures have already strained capacity. Wait times and travel requirements would increase significantly if the millions of people who currently access medication abortion via telehealth were redirected to in-clinic care.
What is the Comstock Act and why does it matter?
The Comstock Act is a 19th-century federal law originally designed to prohibit mailing obscene materials. Some legal advocates are pushing to apply it to abortion pills arguing it already makes mailing mifepristone and misoprostol a federal violation. The Supreme Court has not definitively ruled on this application. If accepted by a court, it would criminalize mail-order abortion pills without requiring any new legislation, making it one of the most significant backdoor legal threats to telehealth abortion access.
If telehealth is restricted, can I still get abortion pills from international providers?
Potentially. International providers like Aid Access operate outside US jurisdiction and may remain accessible in some restriction scenarios. However, the legal risk associated with receiving pills from international sources increases under heightened federal enforcement, and these providers operate without the clinical support infrastructure of domestic licensed services. International providers function as a safety net not a replacement for accessing care through legitimate domestic channels while that option fully exists.
Who would be most affected by a nationwide telehealth abortion restriction?
The impact would fall disproportionately on people in rural areas with no nearby clinic access, low-income individuals who cannot afford to travel for care, people currently in protected states who may not expect to lose access, minors navigating parental notification barriers, and survivors of abuse for whom discreet home-based access is essential. The communities with the least existing healthcare infrastructure would absorb the heaviest burden.
What can I do right now to protect my access?
The most direct action is accessing telehealth abortion care while full protections are in place. Beyond that: learn your state’s specific legal protections, identify abortion funds in your area before you need them, build good digital privacy habits now, and stay informed through reliable reproductive healthcare sources. Acting before restrictions are in place is meaningfully easier than navigating care after they take effect. Explore your current options while the full landscape of protection is still available.
Dr. James Carter is a board-certified physician and lead clinician at Serenity Choice Health, specializing in reproductive health access and medication abortion protocols. With over 20+ years of experience, he combines clinical expertise with patient-centered care to ensure safe, compassionate, and confidential reproductive healthcare.