A few years ago, receiving abortion medication through the mail felt like a distant possibility for most Americans. Today it’s a reality that millions of people have relied on quietly, privately, and without the travel, cost, and logistical burden that in-clinic care requires. Telehealth consultations followed by discreet home delivery have fundamentally changed what abortion access looks like in this country.
But the landscape surrounding abortion pills by mail is shifting faster than almost any other area of healthcare policy. Court decisions, regulatory changes, and legislative efforts at both state and federal levels are creating genuine uncertainty about what access will look like in the years ahead. For anyone who relies on this pathway or might need to in the future understanding what’s at stake and what’s actually likely to change matters enormously.
This guide covers where things stand right now, what legal battles are reshaping the landscape, and what patients and providers can realistically expect going forward.
What Are Mail-Order Abortion Pills and How Do They Work?
Medication abortion the clinical term for what’s commonly called the abortion pill uses two medications taken in sequence to end a pregnancy. The first, mifepristone, blocks the hormone progesterone that the pregnancy needs to continue. The second, misoprostol, taken 24 to 48 hours later, causes the uterus to contract and expel the pregnancy. Together, this combination is over 95% effective when used correctly within the recommended gestational window typically up to 10 to 12 weeks of pregnancy.
The telehealth model works like this: a patient consults with a licensed clinician remotely by video or through a secure messaging platform who reviews their medical history, confirms gestational age, and if appropriate, writes a prescription. That prescription is then filled and mailed directly to the patient in discreet, unmarked packaging. The entire process can happen without the patient ever leaving home.
Understanding exactly how the abortion pill works what each medication does, what to expect during the process, and what follow-up looks like is worth doing before you begin, both for your peace of mind and your safety.
Demand for this model has grown dramatically since 2020, driven by a combination of factors: the COVID-19 pandemic normalized remote healthcare broadly, the Dobbs decision created urgent access gaps in restrictive states, and people who had previously been unaware that telehealth abortion existed discovered it as clinic options disappeared around them. Medication abortion now accounts for the majority of abortions in the United States, a statistic that would have been unimaginable a decade ago.
Why Mail-Order Abortion Pills Have Become a Defining Healthcare Issue
The rise of abortion pills by mail isn’t just a healthcare trend. It’s a direct response to a system that has created increasingly severe barriers to in-person reproductive care.
For someone in a rural area where the nearest abortion clinic may be hundreds of miles away, telehealth abortion is not a convenience. It’s often the only option that doesn’t require taking multiple days off work, arranging childcare, covering travel and lodging costs, and navigating the emotional experience of traveling for care in a state that may be actively hostile to the reason you’re traveling. Telehealth abortion care has closed an access gap that physical infrastructure simply cannot fill in the near term, and arguably not ever given how clinic capacity has contracted since Dobbs.
Privacy is the other dimension that often goes undiscussed. For many people, the ability to receive care at home without appearing in a waiting room, without a recognizable provider name on an insurance statement, without any physical trace of where they’ve been is not a preference but a genuine safety consideration. People in abusive relationships, people in small communities where privacy is difficult, people in states where the legal climate creates fear even around legal behavior for all of these people, mail delivery of abortion medication is meaningfully different from any in-person alternative.
Is It Currently Legal to Receive Abortion Pills by Mail?
This is the question most people ask first, and the honest answer is: it depends on where you are and who is sending the medication.
At the federal level, the FDA approved mifepristone in 2000 and has regulated it through the REMS program ever since. A significant change came in 2021 when the FDA modified the REMS to allow certified prescribers to prescribe mifepristone via telehealth and pharmacies to dispense it by mail removing the previous requirement for in-person dispensing at certified facilities. That change is what made the current telehealth abortion model possible at scale.
State laws layer on top of the federal framework in complex and often contradictory ways. In states where abortion is legal, mailing abortion pills is generally permitted. In states where abortion is banned or severely restricted, receiving mailed abortion medication exists in a legally contested space; the medication itself may not be illegal for a patient to receive, but the act of mailing it from another state creates legal exposure for providers.
Shield law states including Illinois, California, New York, Colorado, and others have specifically addressed this by protecting providers who mail abortion medication to patients in restrictive states. A provider operating from a shield law state cannot have their license revoked or face successful prosecution in their home state for mailing medication to a patient in a restrictive state. You can read a detailed breakdown of how abortion shield laws work and what they specifically protect.
One common misunderstanding worth addressing: the Comstock Act, a 19th-century federal law, has been cited by some advocates as already prohibiting the mailing of abortion pills, without any new legislation required. Most legal scholars consider this application a significant stretch of the original law’s intent, and it has not been enforced in this way. But it represents a genuine legal risk if interpreted aggressively by federal authorities or upheld by a court, and it bears watching.
What Legal Challenges Could Shape the Future of Abortion Pill Access
The legal landscape surrounding medication abortion by mail is genuinely unsettled, and several active threads could pull it in very different directions over the next few years.
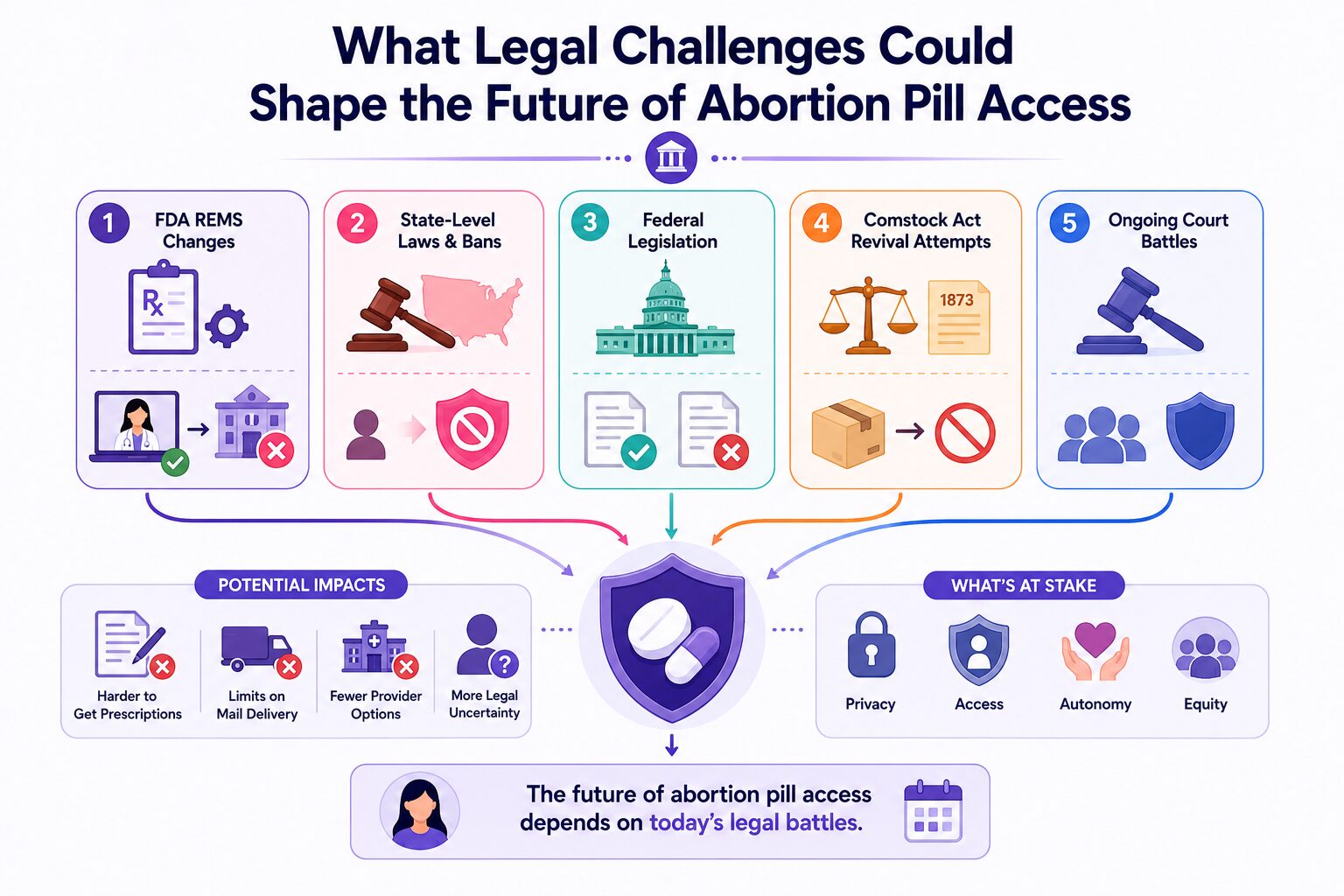
The FDA REMS pathway is the most immediate regulatory pressure point. The current REMS allows telehealth prescribing and mail delivery. A future administration could direct the FDA to tighten those requirements potentially reverting to the pre-2021 standard that required in-person dispensing at certified clinics. This would not ban mifepristone, but it would effectively eliminate the mail-order model for that medication. Critically, this pathway does not require Congressional action; it can happen through the regulatory process alone, making it faster and less predictable than legislation.
State-level legislative efforts continue to test the boundaries of what restrictive states can do to prevent their residents from accessing medication through telehealth providers in other states. Most aggressive proposals attempting to criminalize patients who receive mailed abortion pills, or to hold third parties liable for facilitating access have faced legal challenges. But the legislative pressure is real and ongoing.
Federal legislation remains a longer-term possibility in either direction. A federal law protecting abortion pill access would override state restrictions. A federal restriction or ban would override state shield laws. Neither outcome is imminent given current Congressional arithmetic, but both are possible over a longer horizon, and the direction of federal policy matters enormously for what state-level protections can actually accomplish.
Comstock Act revival attempts represent perhaps the most significant backdoor legal threat. If a court were to accept the argument that the Comstock Act already prohibits mailing abortion medication meaning enforcement could begin without new legislation it would immediately affect every mail-order abortion provider regardless of where they are located or what state shield laws say. This is not the most likely scenario, but it is a real one that providers and legal advocates are monitoring closely.
How Telehealth Could Expand Abortion Access in the Next Decade
Despite the legal headwinds, the underlying trajectory of telehealth as a healthcare delivery model is strongly positive and that trajectory intersects meaningfully with abortion access.
Virtual healthcare has normalized across almost every medical specialty since 2020. Patients are more comfortable with remote consultations, providers have invested in telehealth infrastructure, and regulatory frameworks have adapted in ways that are difficult to fully reverse even when political winds shift. The technological capacity to provide high-quality abortion care remotely including thorough clinical screening, accurate gestational dating guidance, and reliable follow-up has matured considerably.
Multi-state licensing compacts, which allow providers to practice across state lines more easily, are expanding in several healthcare disciplines. If these frameworks extend meaningfully to reproductive healthcare, they could significantly increase the pool of licensed providers able to offer telehealth abortion consultations to patients in underserved areas.
The practical reality is that for the foreseeable future, telehealth and mail delivery represent the most scalable pathway to abortion access in a country where clinic infrastructure has contracted and is unlikely to rapidly expand. Book a confidential appointment with a licensed clinician today while full protections are still in place.
Could States Restrict Mail-Order Abortion Pills Further?
Yes and some are actively trying. Understanding what restriction strategies are actually viable helps separate realistic concern from speculation.
The most enforceable near-term state restriction strategies focus on providers rather than patients. Targeting patients who receive mailed medication is legally and practically difficult; it requires surveillance of mail, proof of what was in a package, and enforcement mechanisms that most states don’t have and couldn’t easily build. Targeting providers is simpler legally, though shield laws in the provider’s home state significantly limit the effectiveness of those efforts.
Interstate commerce questions represent a genuine legal constraint on how far states can go. Federal law governs interstate commerce, which means states have limited authority to regulate what moves across their borders in the mail. The extent to which abortion medication falls under interstate commerce protection is genuinely contested but it is a real legal constraint on state restriction strategies.
The most realistic near-term scenario is not a sudden comprehensive ban but a gradual tightening REMS modification at the federal level, increased state-level targeting of providers, and a legal environment that makes offering telehealth abortion to patients in restrictive states progressively more legally complex for providers. This is why accessing care through established, shield-law-protected providers while current protections are fully intact matters. Our telehealth abortion care service operates within a fully protected legal framework understanding what that means for your care is worth doing before the landscape shifts further.
What the Future Actually Means for Patients
For someone trying to understand what all of this means practically not legally, not politically, but for their own situation a few things are worth internalizing.
Access exists right now in a form that may be more protected than it will be in the future. Acting while full telehealth protections are in place is categorically simpler than navigating care after restrictions tighten. This is not alarmism, it’s a straightforward assessment of the direction legal and regulatory trends are moving.
The type of provider you use matters. A telehealth provider operating from a comprehensive shield law state, with explicit telehealth abortion provisions and established privacy infrastructure, offers meaningfully better legal protection than an unverified international provider or an informal source. Abortion pill access through a licensed provider with proper clinical screening, follow-up support, and legal protection is the standard worth maintaining regardless of what other options exist.
Privacy considerations are becoming more important, not less. As enforcement interest in abortion-related behavior increases in restrictive states, the digital trails that people leave while researching and accessing care become more significant. Medical records held by licensed providers are HIPAA-protected. Search history, location data, and period tracking app data are not. Understanding how to keep your abortion private is increasingly practical preparation, not paranoia.
Reproductive healthcare doesn’t end with abortion care. After completing a medication abortion, many people take the opportunity to revisit their longer-term reproductive health needs. Birth control and contraceptive services are an important part of ongoing reproductive care and accessing them through the same trusted provider creates continuity that matters for your health long-term. Routine STI and STD testing is equally important and often overlooked during periods of reproductive healthcare focus. Women’s primary care services that integrate abortion care, contraception, testing, and general health create the kind of consolidated, private care experience that serves patients most completely and reduces the number of separate providers a patient needs to navigate.
Cost and financial access are real barriers that have real solutions. Medication abortion via telehealth is generally less expensive than in-clinic procedures, but cost remains a barrier for many people. Abortion financial assistance programs exist specifically to address this and knowing they exist before you’re in a time-sensitive situation is genuinely useful.
How Healthcare Providers Are Adapting to a Changing Landscape
The providers and platforms currently operating in this space are not passively waiting to see what regulations emerge. They are actively restructuring how they deliver care in anticipation of a more restrictive environment.
Telehealth platforms are consolidating operations in shield law states, deliberately structuring their legal and clinical infrastructure to maximize the protections those states offer. Multi-state licensing is being pursued aggressively by individual clinicians who want to serve patients across the broadest possible geographic range. Data retention policies are being tightened; providers are limiting what they store, how long they store it, and who can access it, in direct response to the subpoena and investigation risks that a more restrictive environment creates.
For patients, this provider adaptation has a practical implication: not all telehealth abortion providers are equally well-positioned legally. Providers who have deliberately structured their operations around shield law protection, who maintain rigorous data privacy practices, and who offer comprehensive women’s primary care services alongside abortion care are offering something meaningfully different from platforms that haven’t made those investments. In-clinic abortion services remain an important option for patients whose gestational age or medical circumstances make medication abortion less appropriate and providers who offer both pathways create the most complete care experience.
What Abortion Pill Access Could Look Like by 2030
Honest forecasting on this topic requires acknowledging real uncertainty; the legal and political landscape is shifting too quickly for confident predictions. But three scenarios are worth understanding.
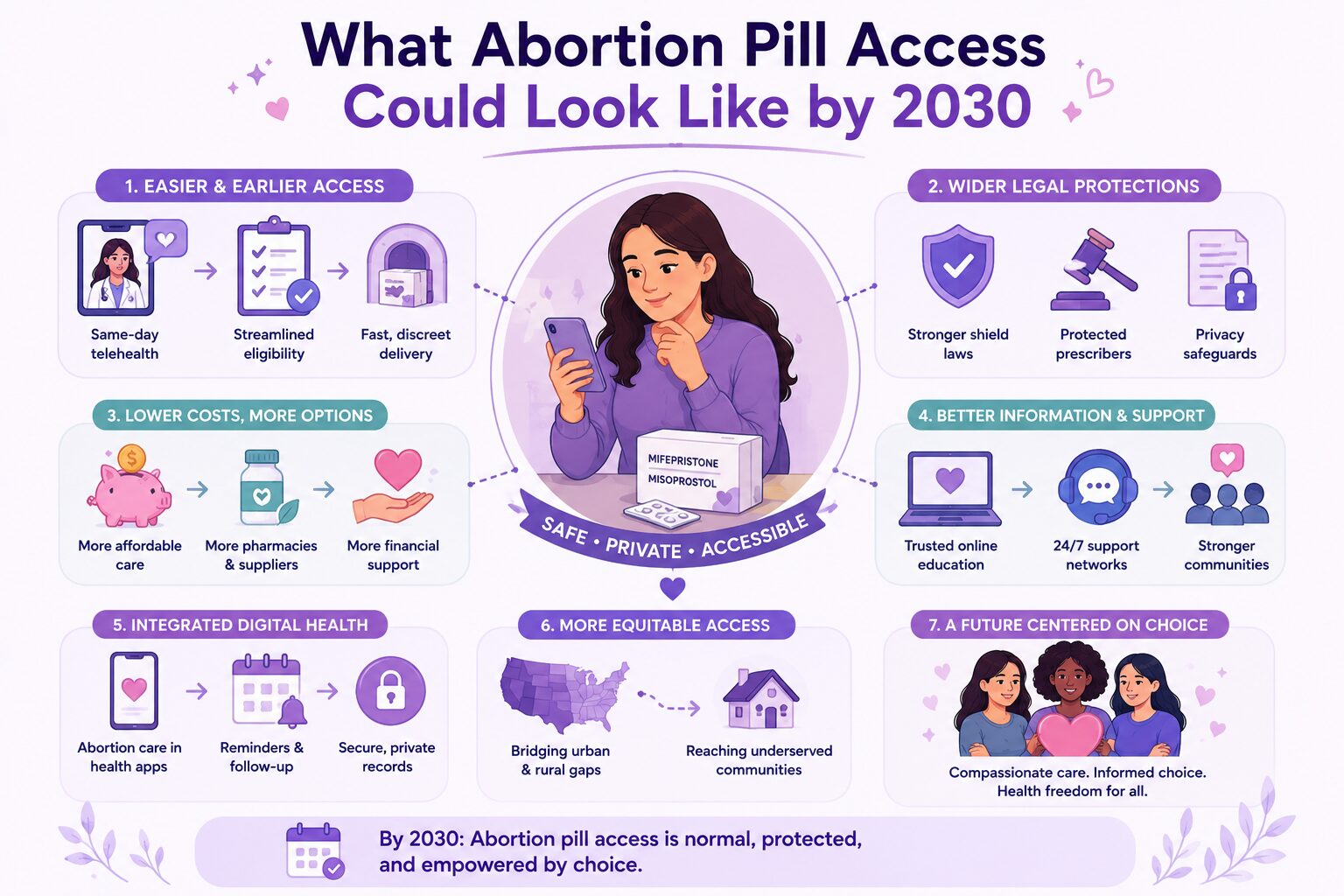
The optimistic scenario involves federal courts and Congressional action protecting telehealth abortion access, shield laws surviving legal challenge, and the telehealth model continuing to expand access for people in both protected and restrictive states. In this scenario, mail-order abortion pills become an increasingly normalized part of the reproductive healthcare landscape as routine as any other telehealth prescription.
The realistic scenario involves incremental tightening REMS modification requiring in-person dispensing for mifepristone, increased legal pressure on providers serving patients in restrictive states, and a gradual reduction in the provider pool willing to operate in the most legally complex environments. In this scenario, access persists but becomes more concentrated in shield law states, more expensive, and more dependent on knowing where to look.
The restrictive scenario involves successful Comstock Act enforcement, federal legislation restricting telehealth abortion, or Supreme Court decisions that significantly limit the legal framework supporting current access. In this scenario, mail-order access contracts dramatically, in-clinic care becomes the primary pathway for most people, and clinic capacity which cannot absorb current medication abortion volume becomes a critical bottleneck.
Most legal and healthcare policy analysts consider the realistic scenario most probable over the next few years with the direction of upcoming election cycles likely to determine whether the trajectory moves toward the optimistic or restrictive end of that spectrum.
What’s consistent across all scenarios: people who access care now, through licensed providers in shield law states, while current protections are fully intact, face the fewest barriers and the most legal protection. Book a confidential appointment to speak with a licensed clinician about your current options or explore whether in-clinic abortion services might be the right fit for your specific situation.
Frequently Asked Questions
What are mail-order abortion pills and are they safe?
Mail-order abortion pills refer to mifepristone and misoprostol, the FDA-approved two-medication regimen for medication abortion prescribed via telehealth and delivered directly to a patient’s home. When obtained through a licensed provider following proper clinical screening, they are safe and effective, with an effectiveness rate above 95% within the recommended gestational window. The safety concern arises with pills obtained from unverified sources without clinical oversight counterfeit or mislabeled medication is a genuine risk when sourced outside legitimate medical channels.
Are abortion pills by mail legal in every state?
No. In states where abortion is legal, mail delivery of prescribed abortion medication is generally permitted. In states where abortion is banned or restricted, receiving mailed abortion medication exists in legally contested territory. Providers operating from shield law states are legally protected from prosecution in their home state for mailing medication to patients in restrictive states but the legal risk profile for both providers and patients varies significantly depending on the specific states involved.
How does telehealth abortion actually work?
A patient consults with a licensed clinician remotely via video or secure messaging who reviews medical history, confirms gestational age, and if appropriate writes a prescription. That prescription is filled and mailed in discreet packaging, typically arriving within a few days. The clinician provides instructions for taking the medication, guidance on what to expect, and follow-up support. The entire process happens without requiring an in-person visit. You can learn more about how telehealth abortion care works through a licensed provider.
Can abortion pills be shipped across state lines legally?
In the current legal environment, yes when shipped by a provider in a shield law state. Federal interstate commerce law governs what moves through the mail across state lines, and most legal scholars argue states have limited authority to restrict interstate mail. Shield laws in the provider’s home state add additional protection by preventing prosecution or licensing action against providers who mail medication to patients in restrictive states. The Comstock Act revival argument, if accepted by a court, could change this, which is why this legal thread is closely monitored.
What is mifepristone and why is it the focus of so many restrictions?
Mifepristone is the first medication in the standard two-drug medication abortion regimen. It was FDA-approved in 2000 and has been used safely in the United States for over two decades. It is the primary target of abortion restriction efforts because it is abortion-specific unlike misoprostol, which has multiple non-abortion medical uses and is correspondingly harder to restrict. Controlling mifepristone access, particularly through the FDA’s REMS program, is the most viable regulatory mechanism for restricting medication abortion without a full legislative ban. Learn more about the abortion pill and how the medication process works through a licensed provider.
Could future laws restrict mail-order abortion pills further?
Yes through several pathways. FDA modification of the mifepristone REMS to require in-person dispensing is the most likely near-term mechanism and doesn’t require Congressional action. Federal legislation, Comstock Act enforcement, and continued state-level pressure on providers are additional pathways. The probability and timeline of each depends heavily on election outcomes, court decisions, and regulatory priorities. Acting while current protections are fully in place rather than waiting to see what changes is the most straightforward way to ensure access is available when you need it. Book a confidential appointment today while full protections remain intact.
Dr. James Carter is a board-certified physician and lead clinician at Serenity Choice Health, specializing in reproductive health access and medication abortion protocols. With over 20+ years of experience, he combines clinical expertise with patient-centered care to ensure safe, compassionate, and confidential reproductive healthcare.