
If you’ve had a potential STI exposure and you’re wondering whether to get tested right now the answer is probably yes, but with an important caveat: when you test matters almost as much as whether you test.
One of the most common and consequential mistakes people make after a potential exposure is getting tested the next day, receiving a negative result, and assuming they’re in the clear. That negative result may mean nothing at all not because the test failed, but because the infection simply wasn’t detectable yet. Testing before an infection reaches detectable levels can give you false reassurance that leads to real harm both to your own health and potentially to partners.
Understanding STI window periods the time between exposure and when a test can reliably detect an infection is genuinely important information. It changes how you interpret your results, when you schedule follow-up testing, and how you protect yourself and others in the meantime.
This guide walks through the testing timeline for the most common STIs, explains what window periods mean in practice, and helps you figure out exactly when to get tested for the most accurate results.
Understanding STI Testing Window Periods
The answer varies by infection which is exactly why a single blanket answer like “wait two weeks” doesn’t serve everyone well. Different STIs become detectable at different points after exposure, and testing too early for any of them risks a false negative result.
A window period is the time between when you were exposed to an infection and when that infection becomes detectable on a standard test. During the window period, the infection may be present and active in your body, you may be able to transmit it to others, but a test will return a negative result because there isn’t yet enough of the virus, bacteria, or antibodies to trigger detection.
Window periods exist for a straightforward biological reason. Most STI tests don’t detect the pathogen itself they detect your immune system’s response to it, in the form of antibodies. Your immune system needs time to generate detectable antibody levels after exposure. Some tests do detect the pathogen directly, which shortens the window but even these have minimum detection thresholds that take time to reach.
The general principle is this: if you’ve had a potential exposure, an initial test is reasonable and can catch some infections in their early detectable stages but a negative result during the window period is not a clean bill of health. Follow-up testing at the appropriate interval for each infection is essential before you can be confident in a negative result.
Our STI and STD testing services are designed to guide you through exactly this process with clinician support to help you understand what to test for, when to test, and how to interpret your results.
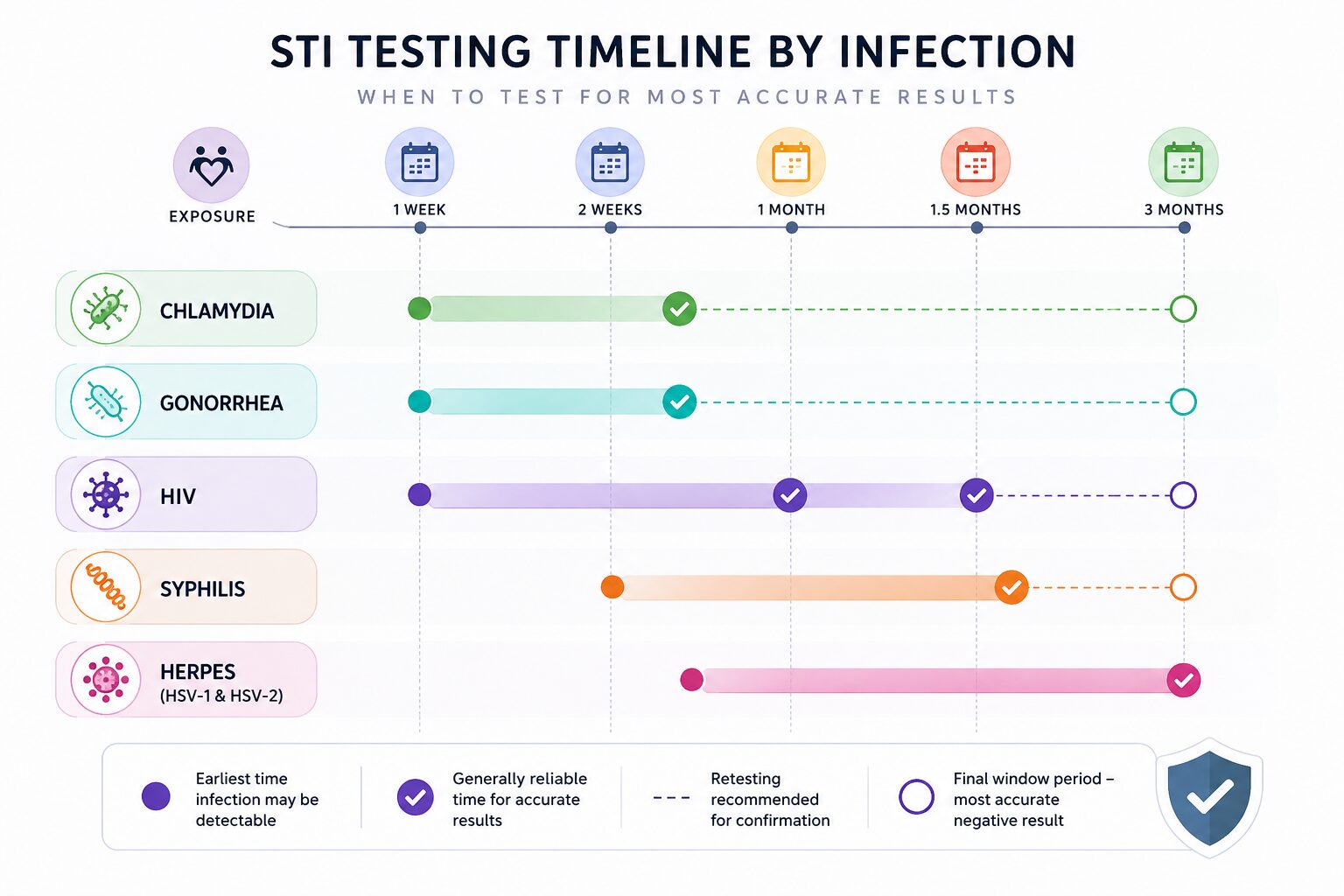
Here is the specific testing timeline for each major STI when you can first test, and when results become most reliable:
Chlamydia Chlamydia can typically be detected 1 to 2 weeks after exposure using nucleic acid amplification tests (NAATs), which detect the bacteria’s genetic material directly. Most guidelines suggest waiting at least 2 weeks after exposure for reliable results. If your initial test is negative but you had a significant exposure, retesting at 3 months is recommended to confirm. Chlamydia is one of the more straightforward infections to detect early the window period is relatively short compared to viral infections.
Gonorrhea Gonorrhea has a similar detection window to chlamydia typically detectable within 1 to 2 weeks using NAAT testing. Results are generally reliable by 2 weeks post-exposure. Like chlamydia, a follow-up test at 3 months is standard practice after a potential high-risk exposure, even with an initial negative result.
HIV HIV has the most complex testing timeline of any common STI, and understanding it matters enormously. There are three main types of HIV tests, each with different window periods:
A 4th generation antigen/antibody test the current standard at most clinics can detect HIV as early as 18 to 45 days after exposure, with most cases detectable by 45 days. This test looks for both HIV antibodies and the p24 antigen, which appears earlier than antibodies. Results are considered conclusive at 45 days for most people, with the CDC recommending a confirmatory test at 90 days for complete certainty.
Antibody-only tests have a longer window up to 90 days and are less commonly used now that 4th generation tests are widely available.
Nucleic acid tests (NATs) can detect HIV as early as 10 to 33 days after exposure and are used in high-risk situations or when early detection is critical but they are more expensive and not used for routine screening.
If you’ve had a high-risk HIV exposure unprotected sex with a partner of unknown status, or needle sharing PEP (post-exposure prophylaxis) is an antiretroviral medication that can prevent HIV infection if started within 72 hours of exposure. This is worth knowing about independently of testing.
Syphilis Syphilis antibodies typically become detectable 3 to 6 weeks after exposure, with most cases detectable by 6 weeks. However, a full 90-day window period is recommended before a negative result can be considered conclusive. The reason for this longer window is that syphilis antibody development can be slower than other infections, and an early test may miss an infection that will become detectable later.
Herpes (HSV-1 and HSV-2) Herpes testing is more complicated than most people expect. Blood tests for herpes detect antibodies, which can take 12 to 16 weeks to develop after exposure meaning herpes is one of the infections with the longest reliable window period. An early negative herpes blood test tells you very little about whether a recent exposure resulted in infection.
If you have active sores or lesions, a swab test of the sore can detect herpes directly and much more quickly often within the first few days of an outbreak. But for exposure without visible symptoms, the 12 to 16 week window applies.
It’s also worth knowing that herpes testing is not typically included in standard STI screening panels you need to specifically request it.
HPV HPV testing is handled differently from other STIs. There is no approved HPV test for people with penises, and for people with cervixes, HPV is detected through cervical screening a Pap smear or combined Pap/HPV co-test rather than through a separate STI test. HPV may not cause detectable cervical changes for months to years after exposure, which is why regular cervical screening at recommended intervals is more relevant than post-exposure testing for this infection.
Trichomoniasis Trichomoniasis can generally be detected within 5 to 28 days after exposure. Most cases are reliably detectable within 2 weeks, making it one of the shorter window period infections.
| Infection | Earliest Detection | Reliable Result | Recommended Retest |
|---|---|---|---|
| Chlamydia | 1–2 weeks | 2 weeks | 3 months |
| Gonorrhea | 1–2 weeks | 2 weeks | 3 months |
| HIV (4th gen) | 18–45 days | 45 days | 90 days |
| Syphilis | 3–6 weeks | 6 weeks | 90 days |
| Herpes | 12–16 weeks | 16 weeks | N/A (swab if symptomatic) |
| Trichomoniasis | 5–28 days | 2 weeks | As needed |
| HPV | N/A | Cervical screening | Per screening guidelines |
Can You Get Tested Immediately After Exposure?
Yes — and in some situations, immediate medical contact after exposure matters for reasons beyond testing.
If you’ve had a potential HIV exposure within the past 72 hours, contacting a healthcare provider immediately about PEP is more urgent than any test. PEP is a 28-day course of antiretroviral medication that can prevent HIV infection from establishing but it must be started within 72 hours of exposure to be effective, and the sooner the better.
For bacterial STIs like chlamydia and gonorrhea, same-day testing is possible, but the results should be understood in context. A negative result within the first few days of exposure means very little the window period hasn’t elapsed and the infection simply may not be detectable yet. However, testing immediately also establishes a baseline if you test negative now and positive in three weeks, that helps establish timing of the infection.
The most important thing to understand about early testing is what a negative result does and doesn’t tell you. A negative result within the window period does not mean you weren’t exposed, doesn’t mean you’re not infected, and doesn’t mean you’re safe to have unprotected sex. It means the test didn’t detect anything at this point in time which is a very different thing.
Booking a confidential appointment with a licensed clinician allows you to discuss your specific exposure, understand which tests are most relevant for your situation, and get guidance on the right testing timeline rather than navigating this alone.
What If You Already Took an STI Test?
If you’ve already tested particularly if you tested within the first few days of a potential exposure the question of how to interpret that result is important.
A negative result within the window period should be treated as inconclusive, not reassuring. This is one of the most common sources of false reassurance in sexual health. People test early, receive a negative result, and proceed as if they’ve been cleared when in fact they’ve simply tested before the infection was detectable.
If you tested too early, the right response is to retest at the appropriate window period for the infection you’re most concerned about. For HIV, that means retesting at 45 days with a 4th generation test and again at 90 days if you want complete certainty. For chlamydia and gonorrhea, retesting at 2 to 3 weeks from exposure provides a much more reliable result than a same-day test.
A positive result at any point even early is meaningful and should be followed up with a clinician promptly. Most bacterial STIs are straightforward to treat with antibiotics when caught early. Our in-clinic abortion services and STI testing include clinician review of results and guidance on next steps so you’re not left trying to interpret results on your own.
Should You Wait for Symptoms Before Getting Tested?
No and this is one of the most important points in this entire guide.
Symptoms are not a reliable trigger for STI testing, for the same reason that asymptomatic infections are so common. The majority of chlamydia cases in women produce no symptoms. A significant proportion of gonorrhea cases go unnoticed. HIV in early infection often produces no symptoms, or symptoms so mild they’re attributed to a cold or flu. Trichomoniasis frequently causes no noticeable discomfort.
Waiting for symptoms before testing means waiting for complications in many cases because by the time symptoms appear, an infection may have been present for weeks or months, and in the case of bacterial STIs, may have already begun causing internal damage.
The correct approach is to test based on exposure and timeline not based on whether you feel anything. If you had a potential exposure, the question is when to test, not whether you should. And the answer to when depends on the window period for the infections you’re most at risk for, not on whether symptoms develop.
Our women’s primary care services integrate STI screening into routine healthcare making it straightforward to stay on top of sexual health without waiting for a reason to be concerned.
What Factors Affect STI Detection Times?
Beyond the specific infection, several factors influence when testing becomes accurate:
The testing method matters significantly. NAAT tests, which detect genetic material from bacteria or viruses directly, have shorter window periods than antibody tests for the same infection. When speed of detection matters, asking your provider which testing method they’re using is worth doing.
Your individual immune response plays a role. Most window period estimates are averages some people develop detectable antibodies faster, others slower. This is part of why confirmatory retesting at the upper end of the window period provides more certainty than testing at the lower end.
The type and intensity of exposure affects both risk and detection considerations. A higher-risk exposure unprotected anal or vaginal sex, for example warrants more thorough and potentially more urgent follow-up than a lower-risk encounter.
Existing immune system factors, including other infections or immune-compromising conditions, can affect how quickly your body generates a detectable response.
At Home STI Testing vs Clinic Testing
At-home STI tests have improved significantly in recent years and offer genuine advantages particularly for people who want privacy or have difficulty accessing a clinic. However, they come with limitations worth understanding.
At-home tests are generally accurate when used correctly and at the right time in the window period. The same window period considerations apply regardless of whether you test at home or in a clinic testing too early produces the same unreliable results either way. Learn more about the benefits of telehealth and how virtual care can support your sexual health needs.
The practical advantage of clinic-based testing is clinical support. A provider can help you understand which tests are most relevant for your specific exposure, advise on timing, interpret results in context, prescribe treatment immediately if a positive result comes back, and recommend follow-up testing where needed. At-home tests give you results but not context.
For routine screening when you feel fine and want to stay on top of your sexual health, at-home tests are a reasonable option. For post exposure testing where you need accurate results and potentially urgent follow-up, clinic-based testing with provider support is the stronger choice. Our telehealth abortion care and broader virtual services make accessing confidential clinical support easier than ever.
When Should You Retest for STIs?
Retesting recommendations vary by situation:
After an early negative result if you tested within the window period and received a negative result, retest at the appropriate interval for the infection you’re most concerned about. For HIV, that’s 45 days (4th generation test) and again at 90 days. For chlamydia and gonorrhea, 2 to 3 weeks from exposure. For syphilis, 6 weeks and again at 90 days.
After treatment for a bacterial STI retesting 3 months after treatment for chlamydia or gonorrhea is recommended to confirm clearance and check for reinfection.
After a new or high-risk exposure even if you have recent negative results, a new potential exposure warrants a new testing cycle with appropriate window period timing.
For routine maintenance sexually active people with multiple partners benefit from regular STI screening every 3 to 6 months, regardless of symptoms or specific exposures.
Common STI Testing Mistakes
Testing too soon and treating the result as conclusive. A negative result within the window period is inconclusive not reassuring. This is the single most common STI testing mistake and the one with the most serious consequences.
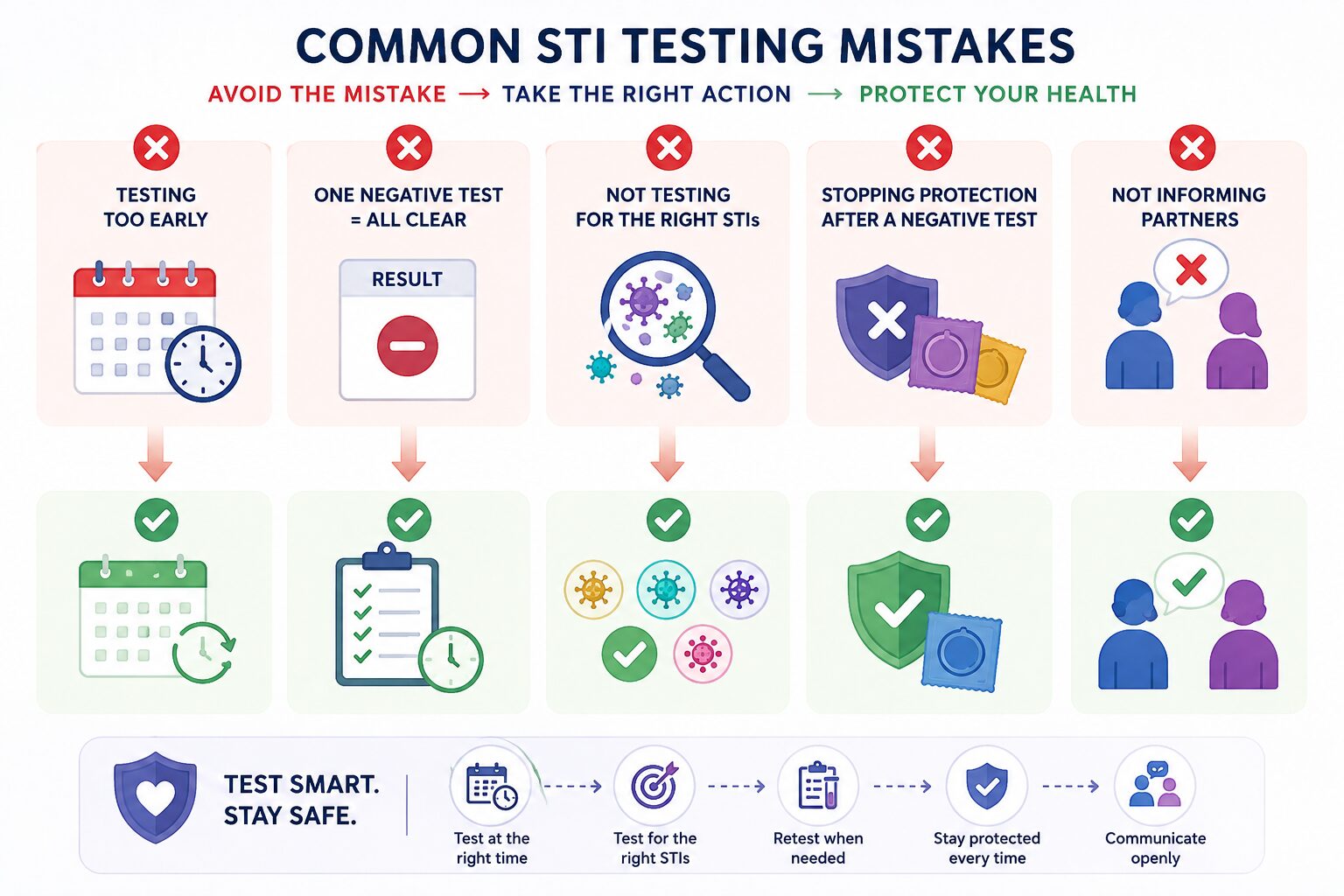
Assuming no symptoms means no infection. Many of the most common STIs produce no symptoms, particularly in early stages. Feeling fine is not evidence of a negative status.
Skipping follow-up testing after an early negative. An initial negative after exposure is the beginning of a testing process, not the end. Follow-up at the appropriate window period is essential for accuracy.
Not testing for the right infections. Standard STI panels don’t always include every infection. Herpes is frequently not included unless specifically requested. HPV is detected through cervical screening, not a standard STI swab. Knowing what your test covers and what it doesn’t — matters.
Testing once and assuming permanent coverage. A negative test result tells you about your status at a specific point in time. It says nothing about future exposures. Regular, routine screening is what keeps you informed over time.
How to Protect Yourself While Waiting for Results
The period between testing and receiving results and between initial testing and follow-up testing requires thoughtful decisions about protecting yourself and partners.
Using barrier protection consistently during this period is the most straightforward protective measure. Communicating with partners about potential exposure while emotionally challenging is an important part of responsible sexual health practice. Partners who may have been exposed deserve the opportunity to get tested themselves.
Managing anxiety during the waiting period is genuinely difficult for many people. Understanding that a test is the most productive thing you can do — and that most STIs are treatable when caught early can help reframe the waiting period constructively.
Accessing comprehensive reproductive and sexual healthcare through a provider who takes your concerns seriously makes a real difference. Our birth control and contraceptive services and abortion pill information create a complete care environment where sexual health is treated as the routine, important part of overall health that it is not something to manage in crisis moments only.
Frequently Asked Questions
How soon after exposure can an STI be detected?
It depends on the infection. Chlamydia and gonorrhea become detectable within 1 to 2 weeks using NAAT testing. HIV becomes detectable at 18 to 45 days with a 4th generation test, with conclusive results at 90 days. Syphilis becomes reliably detectable at 6 weeks, with a 90-day window for complete certainty. Herpes antibodies take 12 to 16 weeks to develop. Trichomoniasis is generally detectable within 2 weeks. Testing before these windows elapse risks a false negative result.
Can I get tested for STIs the day after exposure?
You can but the results will be largely inconclusive for most infections. The one situation where same-day or next-day contact with a provider is genuinely urgent is potential HIV exposure, where PEP must be started within 72 hours to be effective. For all other STIs, immediate testing establishes a baseline but should be followed by retesting at the appropriate window period before a negative result can be trusted. Our STI and STD testing services include clinician guidance on timing so you understand exactly when to test and retest.
What happens if I test too early?
A test taken before the window period has elapsed may return a false negative meaning the infection is present but not yet at detectable levels. If you test too early and receive a negative result, you should retest at the appropriate window period for the infections you were screened for. Do not treat an early negative as conclusive. If you’re unsure whether you tested too early, booking a confidential appointment with a clinician can help you interpret your results accurately. You can also learn more about protecting your health privacy when seeking sensitive medical care.
How accurate are STI tests immediately after exposure?
Accuracy immediately after exposure is low for most infections specifically because most tests haven’t had time to detect the infection. Accuracy increases over time as the infection reaches detectable levels. By the end of the recommended window period for each infection, modern STI tests are highly accurate 99% or above for most infections when used correctly.
Should I retest after a negative STI result?
Yes if your initial test was taken within the window period, retesting is essential before you can be confident in a negative result. If your initial test was taken after the full window period elapsed, retesting is still recommended after any new potential exposure, and routine screening every 3 to 6 months is recommended for sexually active people with multiple partners.
Which STI has the longest window period?
Herpes has one of the longest window periods for blood-based antibody testing — up to 12 to 16 weeks. Syphilis and HIV also have extended window periods up to 90 days for complete certainty with standard testing. This is why these infections specifically require follow-up testing at 3 months after potential exposure, even if earlier tests come back negative. Our women’s primary care services include comprehensive screening protocols that account for these different window periods ensuring you’re tested at the right time for the most accurate results.
Dr. James Carter is a board-certified physician and lead clinician at Serenity Choice Health, specializing in reproductive health access and medication abortion protocols. With over 20+ years of experience, he combines clinical expertise with patient-centered care to ensure safe, compassionate, and confidential reproductive healthcare.