At first glance, the trend seems contradictory. Across the United States, dozens of states have enacted significant restrictions on abortion access since the Dobbs decision in 2022. Clinics have closed. Legal penalties for providers have increased. The political environment around reproductive healthcare has become more hostile than at any point in the past five decades.
And yet medication abortion the use of pills to end a pregnancy continues to grow. Not just persist, but actively increase as a share of all abortion care in America.
How does that happen? Why aren’t stricter state laws translating into reduced abortion rates? And what does this trend reveal about how healthcare, technology, patient behavior, and policy are intersecting in ways that lawmakers may not have anticipated?
This piece works through those questions honestly, without political framing and without oversimplification. The forces driving the rise of abortion pill use despite state bans are real, complex, and worth understanding whether you’re someone navigating your own healthcare decisions, a provider trying to understand patient needs, or simply someone trying to make sense of a trend that seems to defy easy explanation.
What Is Medication Abortion and Why Has It Become So Widely Used?
Medication abortion uses two drugs taken in sequence to end a pregnancy. The first, mifepristone, works by blocking progesterone, the hormone the pregnancy requires to develop. The second, misoprostol, taken 24 to 48 hours later, causes uterine contractions that expel the pregnancy. When used correctly within the recommended gestational window typically up to 10 to 12 weeks the combination is over 95% effective.
Understanding exactly how the abortion pill works what each medication does, what the experience involves, and what follow-up looks like helps clarify why so many people prefer this option when it’s available to them.
Before diving into why medication abortion continues to rise despite restrictions, it’s worth understanding why patients began preferring it in the first place. Several factors have driven adoption over the past decade.
Privacy is significant. Medication abortion can happen at home, on a patient’s own timeline, without a waiting room, without a recognizable provider name on a bank statement, and without any public trace of where they’ve been or why. For people in small communities, in abusive relationships, or in states where the social and legal climate makes seeking any reproductive care feel risky, that privacy isn’t a minor convenience it’s a meaningful safety consideration.
Cost matters too. Medication abortion is generally less expensive than in-clinic procedural abortion, and the telehealth model has reduced ancillary costs: no transportation, no time off work, no childcare needed while traveling to a clinic. For lower-income patients who face the most severe access barriers, those cost differences are real and significant.
And for many patients, the experience itself feels more manageable. Being at home, in a familiar environment, with control over timing and setting, is genuinely preferable to navigating a clinical environment, particularly one that may require traveling through hostile territory to reach.
Why Medication Abortion Continues to Rise Despite State Bans
The core reason restrictions haven’t reduced medication abortion rates is straightforward, even if its implications are complex: restricting legal access to a service doesn’t automatically reduce demand for that service. It changes how people access it.
This is not a new phenomenon in healthcare or in social policy. Decades of research on drug prohibition, alcohol prohibition, and restrictions on various medical services consistently show the same pattern: when access is restricted, demand doesn’t disappear. It finds alternative pathways.
What’s different about the current medication abortion landscape is that the alternative pathways are unusually viable. Telehealth technology, shield law protections, mail delivery infrastructure, and a growing network of licensed providers specifically organized to serve patients in restrictive states have created a system that is genuinely functional, not a dangerous underground network, but a legally operating, medically supervised alternative to in-state clinic access.
Healthcare researchers have observed something else important: restrictions don’t affect all patients equally. Patients with financial resources, flexibility, and access to information adapt most easily they travel, they find telehealth providers, they access care in protected states. Patients with the fewest resources face the most severe consequences of restriction. This creates a demographic pattern in who is most affected by state bans that is distinct from who is most affected by the overall trend in medication abortion access.
The result is a situation where medication abortion rates among people who can access telehealth services or travel for care have continued to grow, even as in-state clinic-based abortion rates have dropped in restrictive states. The aggregate national trend continues upward because the access pathways that exist are reaching people they weren’t reaching before while clinic-based care has contracted in some areas.
How Telehealth Transformed the Entire Equation
No single factor has done more to sustain and grow medication abortion access in the face of state-level restrictions than telehealth. It changed the geography of care in a fundamental way meaning where a patient lives no longer determines what care they can access, at least within the current legal framework.
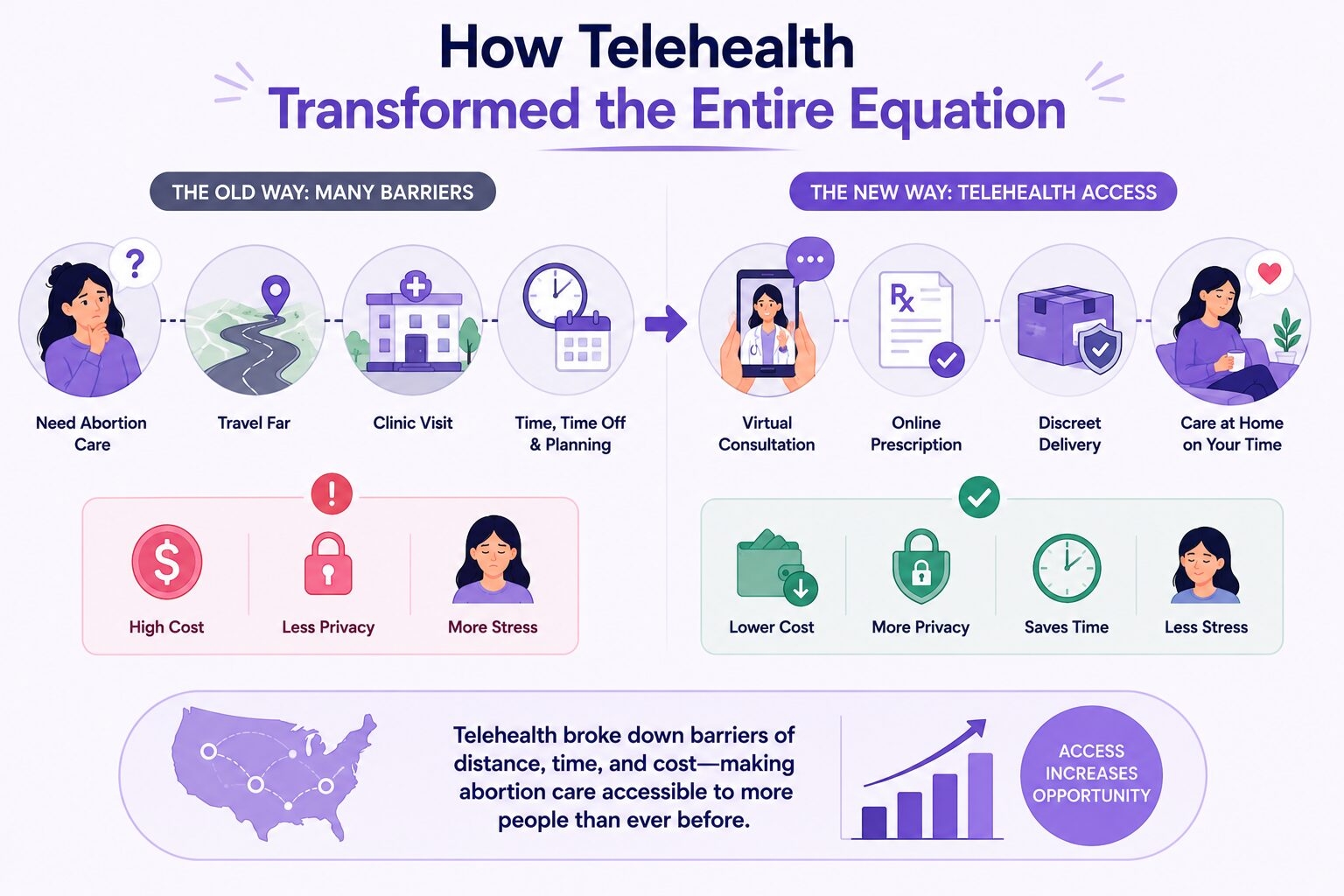
Telehealth abortion care works through a remote consultation with a licensed clinician who reviews the patient’s medical history, confirms gestational age, and if appropriate writes a prescription that is filled and mailed in discreet packaging. The patient never leaves home. No clinic appointment, no travel, no waiting room.
For patients in rural areas where the nearest abortion provider might be three or four hours away, this is transformative. For patients in restrictive states who can access a provider licensed in a shield law state, it creates access that simply didn’t exist in any practical sense before telehealth became viable at scale.
The COVID-19 pandemic accelerated telehealth adoption across all areas of medicine, and the infrastructure that was built during that period in technology, in provider training, in patient comfort with remote consultations benefited telehealth abortion services directly. Patients who might have been unfamiliar with or hesitant about virtual healthcare became comfortable with it rapidly, and that comfort has persisted.
Younger patients in particular have driven significant telehealth adoption in reproductive care. A generation that manages most of its healthcare navigation digitally researching symptoms online, communicating with providers through apps, managing prescriptions through digital platforms approaches telehealth abortion not as a workaround but as the natural format for healthcare delivery. This generational shift in healthcare consumer expectations is one of the structural forces sustaining medication abortion growth that policy restrictions are unlikely to reverse.
Privacy as a Healthcare Driver
Privacy concerns have historically been underweighted in healthcare policy discussions treated as a secondary preference rather than a primary driver of patient behavior. The rise of medication abortion has made clear that privacy is actually a central consideration for a significant portion of patients seeking reproductive care.
The ability to manage an abortion at home, without creating institutional records that flow through insurance systems, without appearing at a facility that can be identified by location data, and without involving anyone else in the decision unless the patient chooses to, is genuinely valuable to a large segment of patients. It’s not just about stigma, though stigma is real. It’s about safety, autonomy, and control over one’s own medical information.
Understanding how to keep your abortion private what protections exist, what risks remain, and what steps patients can take to protect their information has become an important part of informed reproductive healthcare decision-making, particularly in states with restrictive legal environments.
The privacy dimension also explains something important about patient behavior: people who might have accessed in-clinic care when clinics were more available have sometimes actively chosen medication abortion through telehealth even when in-clinic options remain available. The preference isn’t only driven by access barriers it’s driven by genuine patient preference for a more private, home-based experience.
Cost and Convenience The Underappreciated Drivers
Policy discussions about abortion access tend to focus on legal barriers. But the practical, logistical barriers that medication abortion addresses cost, time, transportation, childcare are often equally significant in determining whether someone can actually access care.
Consider what in-clinic abortion access requires for someone without local options: time off work (often without pay), transportation costs, potentially overnight accommodation, childcare arrangements for existing children, and all of this on top of the cost of the procedure itself. Research consistently shows that these logistical barriers prevent a significant number of people from accessing care they are legally entitled to, in states where abortion is legal, simply because the practical requirements are unmanageable.
Medication abortion through telehealth eliminates most of those barriers. A consultation that happens at home, during a lunch break or after the children are in bed, followed by medication arriving in the mail this is not a comparable logistical burden to traveling for in-clinic care.
Abortion financial assistance programs exist specifically to help with cost barriers and for patients who need them, knowing about these resources before facing a time-sensitive situation is genuinely useful preparation.
The convenience factor also intersects with the earliness of care. Medication abortion is most effective earliest in pregnancy. A pathway that allows someone to access care quickly without scheduling delays, travel planning, or clinic appointment availability constraints means more people access care at gestational ages where medication abortion is most appropriate and most effective. This creates a positive feedback loop: accessible medication abortion means earlier care, which means higher effectiveness rates, which increases patient preference for the option.
How Mail-Order Abortion Pills Extended the Geographic Reach
The logistics of mail delivery have proven to be one of the most effective mechanisms for extending medication abortion access beyond the boundaries of what in-person care could reach.


A licensed provider in a shield law state can prescribe abortion medication to a patient anywhere in the country and that medication arrives in discreet, unmarked packaging within days. The patient doesn’t need to be near a clinic, near a major city, or in a state where abortion is legal. The geographic reach of mail-order abortion pills is effectively national, constrained primarily by the legal framework surrounding interstate prescribing rather than by physical infrastructure.
Accessing safe, verified abortion pills online through a licensed provider rather than through unverified sources — is the standard that patients and advocates consistently emphasize. The safety and effectiveness of medication abortion are well-established when the medication is obtained through proper clinical channels. The risks arise primarily when patients turn to unverified sources because legitimate channels feel inaccessible.
The growth of mail-order access has also created a competitive dynamic among providers that has generally benefited patients driving investment in better telehealth platforms, more responsive clinical support, stronger privacy infrastructure, and more patient-centered care models.
What Shield Laws Have Made Possible
The legal infrastructure that makes telehealth abortion viable across state lines rests substantially on shield law protections in states like Illinois, California, New York, and Colorado. These laws protect providers from prosecution or licensing action in their home state based on care they provide to patients in restrictive states creating the legal framework within which cross-state telehealth abortion operates.
Understanding how abortion shield laws work what they protect, what their limits are, and how they interact with federal law is an important context for anyone seeking care through telehealth providers. Shield laws are one of the primary reasons that medication abortion access has remained viable at scale despite growing state-level restrictions.
They also represent genuinely novel legal development states actively creating infrastructure to resist other states’ enforcement efforts and protect cross-border care. The constitutional questions this raises are not fully resolved, and the future of shield law protections under potential federal action remains uncertain. But in the current legal environment, they are functioning as intended, and their existence is a significant factor in why medication abortion rates have not declined in line with what state-level restrictions might have predicted.
What the Future of Medication Abortion Access Looks Like
The forces driving medication abortion growth, telehealth technology, mail delivery infrastructure, shield law protections, patient preference for private home-based care, generational shifts in healthcare consumption are structural. They are not easily reversed by state-level policy changes, and they represent genuine shifts in how healthcare is delivered and consumed.
The most significant near-term uncertainty is at the federal level specifically, whether the FDA’s REMS program for mifepristone will be tightened to require in-person dispensing again, and whether federal enforcement of the Comstock Act will be pursued in ways that target mail delivery of abortion medication. Either of these developments would meaningfully constrain the current model.
Booking a confidential appointment with a licensed clinician to understand your current options in your specific situation is the most direct step available to patients who want to ensure access while current protections are fully in place.
Reproductive healthcare extends beyond abortion care. Birth control and contraceptive services are an important part of ongoing reproductive health and the same telehealth model that has expanded abortion access is increasingly making contraception, STI and STD testing, and comprehensive women’s primary care services more accessible for patients who previously lacked convenient, private options.
The broader arc of this trend points toward a healthcare landscape where reproductive care is increasingly decentralized, digitally delivered, and accessible in ways that don’t depend on proximity to a physical clinic. State-level restrictions have not reversed this arc they have, in some cases, accelerated it, by creating urgency among providers and patients to develop and adopt alternatives. Whether federal action will succeed in constraining it further remains the central open question for the years ahead.
Access is available now. Our telehealth abortion care service connects you with licensed clinicians in a fully protected legal environment confidentially, privately, and without requiring travel. Book your appointment today while full protections remain in place. For patients who prefer or require in-person care, in-clinic abortion services remain available as well.
Frequently Asked Questions
Why is medication abortion continuing to increase despite state bans?
Restricting legal access to a service reduces availability but doesn’t automatically reduce demand. When in-clinic access is restricted, patients find alternative pathways telehealth services, mail-order prescriptions from providers in shield law states, and interstate travel for care. The telehealth infrastructure that exists today is functional, medically supervised, and legally protected in shield law states, which means restrictions have redirected rather than eliminated access for many patients. The aggregate national trend in medication abortion continues upward because new access pathways are reaching patients who previously had no viable options.
What factors are most responsible for driving abortion pill use growth?
Several converging factors drive the trend. Telehealth technology has removed geographic barriers to access. Mail delivery has extended the reach of licensed providers across state lines. Shield law protections have created legal infrastructure supporting cross-state care. Patient preference for private, home-based care has proven to be a genuine and significant driver not just a response to access barriers but an active preference. Cost and logistical advantages of medication abortion over in-clinic care have also accelerated adoption, particularly for patients with limited flexibility around work, childcare, and travel.
How does telehealth affect medication abortion access in restrictive states?
Telehealth allows patients to consult with licensed providers in shield law states remotely, receive a prescription, and have medication mailed to them without crossing state lines or visiting a clinic. This pathway is legally protected for providers operating in shield law states and has created functional access in geographic areas where in-person care is unavailable. The legal risk profile for patients varies by state, but provider-side protections in shield law states are robust under current law. Learn more about how telehealth abortion care works through a licensed provider.
Why do many patients actively prefer medication abortion over in-clinic procedures?
Patient preference for medication abortion extends well beyond access barriers. Privacy, the ability to manage an abortion at home without institutional records flowing through insurance systems or requiring a clinic visit is a primary driver for many patients. The ability to control timing and setting matters too. Cost advantages, the elimination of travel requirements, and comfort with a process that feels more private and autonomous are all genuine preference factors, not just workarounds. For patients who have both options available to them, medication abortion is increasingly the preferred choice.
What role do mail-order abortion pills play in the access landscape?
Mail delivery of abortion medication has extended the geographic reach of licensed providers to patients anywhere in the country regardless of proximity to a clinic. A licensed provider in a shield law state can prescribe and mail medication to a patient in a restrictive state, in discreet packaging, within days of a telehealth consultation. This has created functional access for patients in rural areas and restrictive states who had no viable in-person option. Accessing safe, verified abortion pills online through a licensed provider rather than unverified sources remains the standard for safe and effective care.
How have abortion restrictions actually changed patient behavior?
Restrictions have primarily changed how patients access care rather than whether they seek it. Patients with resources and information have shifted to telehealth services and interstate travel. Patients without those resources face more severe consequences: genuine barriers that result in delayed care or inability to access care at all. The demographic pattern of who is most affected by restrictions is distinct from the overall national trend: restrictions disproportionately affect lower-income patients in rural areas with limited flexibility, while patients with more resources have adapted by using telehealth, mail-order access, and travel. Book a confidential appointment to discuss your specific options with a licensed clinician.
Dr. James Carter is a board-certified physician and lead clinician at Serenity Choice Health, specializing in reproductive health access and medication abortion protocols. With over 20+ years of experience, he combines clinical expertise with patient-centered care to ensure safe, compassionate, and confidential reproductive healthcare.