
When a pregnancy reaches the second trimester, abortion care requires more planning, more medical expertise, and more emotional support. But it remains safe, legal in many states, and fully supported by established medical guidelines. If you or someone you care about is navigating this decision, understanding what second trimester abortion actually involves the procedures, the preparation, and the recovery can make a significant difference in how prepared and supported you feel.
This guide covers everything you need to know about second trimester abortion options from 14 to 24 weeks, written in plain language with clinical accuracy.
What Is a Second Trimester Abortion?
A second trimester abortion is a procedure that ends a pregnancy between 13 and 27 weeks of gestation. Most clinics that provide second trimester care offer services between 14 and 24 weeks. Beyond 24 weeks, care becomes more specialized and is typically limited to cases involving serious fetal anomalies or significant health risks to the pregnant person.
The second trimester is distinct from the first because the pregnancy is more developed, the uterus is larger, and the cervix requires more preparation before a procedure can safely take place. These factors mean that second trimester procedures take longer to prepare for and require a higher level of clinical expertise but they do not make the procedures unsafe. When performed by trained providers, second trimester abortions are medically safe with a very low rate of serious complications.
Why Do People Have Second Trimester Abortions?
People seek abortion care in the second trimester for a wide range of reasons. Understanding these reasons matters because it shapes how providers approach care and why non-judgmental support is central to the experience.
Common reasons include late detection of pregnancy, which is more common than many people realize and can occur due to irregular periods, minimal symptoms, or other health conditions that mask pregnancy signs. Fetal anomalies diagnosed during second trimester screening such as chromosomal conditions or structural abnormalities are another significant reason. Health complications affecting the pregnant person, including conditions that worsen with pregnancy, may also make second trimester abortion medically necessary.
Delayed access to care is a structural factor that affects many people. Financial barriers, lack of nearby providers, insurance delays, and the time required to travel to a clinic particularly for people in states with restricted access can push care into the second trimester even when a decision was made earlier. Personal circumstances, including changes in relationship status, housing instability, or a new diagnosis, also factor into the timing of these decisions.
Each situation is unique. Medical providers who specialize in this care understand that and approach every patient without judgment. Learn more about why people have abortions and the full range of circumstances that lead people to seek care.
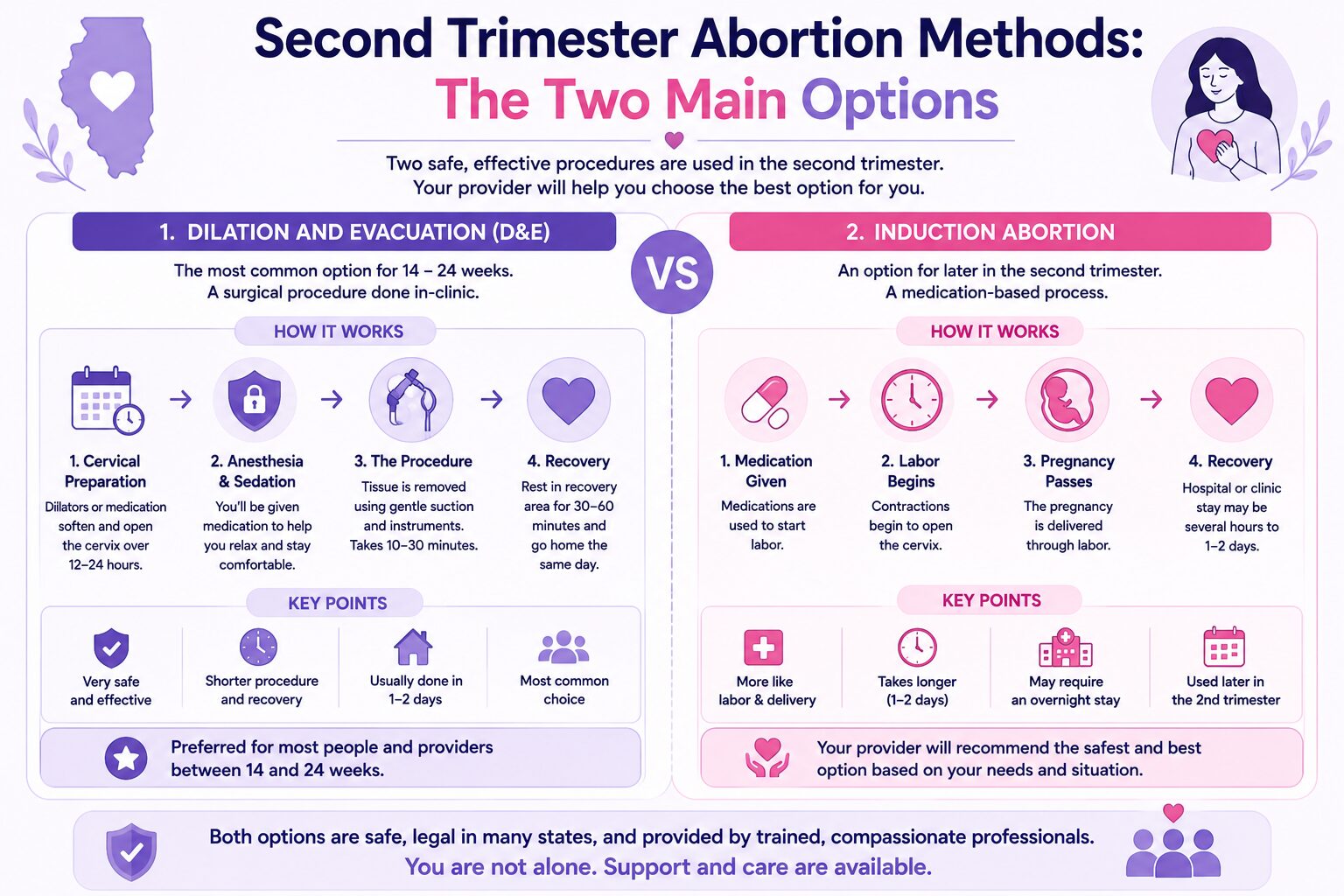
Second Trimester Abortion Methods: The Two Main Options
There are two primary procedures used for second trimester abortion: Dilation and Evacuation (D&E) and induction abortion. The appropriate method depends on gestational age, your medical history, clinic capabilities, and in some cases personal preference.
Dilation and Evacuation (D&E)
D&E is the most widely used second trimester abortion procedure and is considered the safest and most effective method for pregnancies between 14 and 24 weeks. It is an in-clinic surgical procedure performed by a trained provider and is typically completed in a single visit or over two days depending on the level of cervical preparation required.
How D&E Works
Cervical Preparation
Before the procedure itself, the cervix must be gradually dilated to allow the procedure to be performed safely. This is done using osmotic dilators, slender rods made of seaweed-derived material (laminaria) or synthetic material (Dilapan) that are placed inside the cervical opening and slowly absorb moisture, expanding over several hours. Misoprostol, a medication that softens and opens the cervix, may also be used.
Cervical preparation typically begins the day before the procedure and may take 12 to 24 hours. For pregnancies further along in the second trimester, preparation may take longer or require two rounds. This step is essential for safety it reduces the risk of cervical injury during the procedure itself.
Anesthesia and Sedation
On the day of the procedure, you will be offered pain management and sedation options. These typically include local anesthesia (numbing medication applied to the cervix), IV sedation (a relaxing medication given through an IV that reduces awareness and discomfort), or in some clinics, general anesthesia. Most people having a D&E choose IV sedation, which keeps them comfortable and calm without requiring full unconsciousness.
Your provider will discuss your options and recommend the most appropriate level of sedation based on your health history and gestational age. Learn more about anesthesia options for surgical abortion to understand what to expect.
The Procedure
The D&E procedure itself typically takes between 10 and 30 minutes. Your provider uses a combination of gentle suction and specialized surgical instruments to remove the pregnancy tissue from the uterus. Ultrasound guidance is used throughout to ensure the procedure is performed accurately and safely.
Recovery
After the procedure, you will rest in a recovery area for 30 to 60 minutes while staff monitor your vital signs and comfort. Most people are able to go home the same day. Physical recovery for a D&E is generally faster than for induction abortion, with most people returning to normal activities within a few days.
Why D&E Is the Most Common Choice
D&E is preferred by most providers and patients because it is fast, predictable, and has a well-established safety record. The procedure is completed in a controlled clinical setting, pain is manageable with sedation, and the physical recovery period is relatively short. For these reasons, D&E is the standard of care for second trimester abortion in the majority of clinical settings. You can read more in our detailed guide on surgical abortion procedures explained.
Induction Abortion
Induction abortion is a second method used primarily in specific clinical circumstances. Rather than a surgical procedure, induction abortion uses medication to stimulate uterine contractions, causing the pregnancy to be delivered vaginally similar in process to labor and delivery.
How Induction Abortion Works
Medications typically misoprostol, mifepristone, or a combination are administered to initiate contractions. The cervix softens and dilates gradually as contractions progress, and the pregnancy is delivered over a period that typically ranges from 12 to 48 hours. The process takes place in a hospital setting with continuous nursing support and monitoring throughout.
When Induction Is Used
Induction abortion is generally recommended in specific circumstances rather than as a first-line option. These include certain fetal conditions where intact delivery is preferred for diagnostic or personal reasons, specific maternal health conditions that make surgical procedures higher risk, and gestational ages or fetal sizes where D&E may be technically more complex. Some people also choose induction for personal or emotional reasons related to the nature of the delivery process.
What to Expect During Induction
Because induction abortion is a longer process, it requires a hospital stay and involves a more physically and emotionally demanding experience than D&E. Pain management is available and important most providers offer epidural analgesia or IV pain medication to keep patients comfortable throughout the process. Nursing staff remain present to provide both medical monitoring and emotional support.
You can read a full breakdown of the induction abortion complete process guide for more detailed information.
Comparing D&E and Induction Abortion
| Feature | D&E | Induction Abortion |
| Duration | 10–30 minutes | 12–48 hours |
| Setting | Clinic or outpatient | Hospital |
| Pain level | Mild to moderate with sedation | Moderate to high, managed with medication |
| Recovery | 1–3 days | Several days to 1 week |
| Most common use | 14–24 weeks, most cases | Specific medical or personal circumstances |
| Same-day discharge | Usually yes | No |
How to Prepare for a Second Trimester Abortion
Preparation for a second trimester abortion involves both clinical steps your provider will take and practical steps you can take to make the experience as manageable as possible.
Clinical Preparation
Before your procedure, your provider will perform an ultrasound to confirm gestational age and the position of the pregnancy. Blood tests will check your blood type, Rh factor, and other relevant health markers. Your medical history will be reviewed to identify any factors that may affect anesthesia or sedation choices, and you will receive detailed instructions about eating, drinking, and medications before the procedure. Consent forms will be reviewed and signed.
If you have a negative blood type, you will receive an Rh immunoglobulin injection to prevent complications in future pregnancies.
What You Can Do to Prepare
Wear comfortable, loose-fitting clothing on the day of your procedure. Arrange for someone to drive you home and stay with you for the first several hours, as sedation affects your ability to drive safely. Bring a sanitary pad, a water bottle, and a light snack for after the procedure. Plan to rest for the remainder of the day and ideally take the following day off from work or other responsibilities if possible.
Emotional preparation matters too. Talking to a trusted person, a counselor, or a patient advocate before your appointment can help reduce anxiety and ensure you feel supported going in. Our abortion pain management guide explains what to expect physically so there are no surprises on the day.
If you are scheduling care, book an appointment with our team to discuss your options and get a clear plan in place before your procedure date.
What to Expect During Recovery
Recovery from a second trimester abortion varies depending on the procedure and your individual health, but most people follow a similar general pattern.

Immediately After the Procedure
In the hours following a D&E, it is normal to experience mild to moderate cramping, light to moderate vaginal bleeding, fatigue, and some emotional heaviness or relief. These are all expected responses and do not indicate a complication. Nurses will monitor you before discharge and provide written aftercare instructions.
The First Week
Bleeding typically continues for one to two weeks following the procedure, gradually decreasing in flow. Cramping usually improves significantly within the first 48 hours. During the first week, it is important to avoid inserting anything into the vagina including tampons and having penetrative sex to reduce the risk of infection while the cervix heals. Gentle walking is fine, but strenuous exercise and heavy lifting should be avoided.
Over-the-counter pain relievers such as ibuprofen are effective for managing cramping during recovery. Your provider may also prescribe additional medication if needed.
Follow-Up Care
Most providers schedule a follow-up appointment one to two weeks after the procedure to confirm that the uterus has returned to its normal state and that healing is progressing well. This visit is important and should not be skipped. Read our full second trimester abortion recovery guide for a week-by-week breakdown of what to expect.
When to Contact Your Provider
While serious complications are rare, there are specific signs that require prompt medical attention. Contact your provider or go to an emergency room if you experience soaking more than two pads per hour for two or more hours, fever above 101°F, severe abdominal pain that is not relieved by pain medication, foul-smelling vaginal discharge, or no bleeding at all within 24 hours of the procedure.
Emotional Recovery After a Second Trimester Abortion
The emotional experience of a second trimester abortion is individual and cannot be predicted or prescribed. Some people feel relief, some feel grief, and many feel both at different times. There is no correct emotional response, and whatever you feel is valid.
Second trimester abortions particularly those involving wanted pregnancies affected by fetal anomalies or health complications can involve a grief process that is distinct from first trimester experiences. Giving yourself time and space to process, and having access to the right support, makes a meaningful difference.
Support options include talking to a trusted friend or family member, connecting with a counselor or therapist who has experience in reproductive health, or reaching out to a patient advocate through your clinic. Our guide on how to recover emotionally after an abortion offers practical guidance for the weeks following your procedure. Our women’s primary care services also include referrals to mental health support as part of ongoing reproductive healthcare.
Reproductive Health After a Second Trimester Abortion
Fertility typically returns quickly after a second trimester abortion often within two to four weeks. If you do not wish to become pregnant again immediately, it is important to discuss contraception with your provider before or at your follow-up appointment. Contraception can often be started on the same day as the procedure.
Our birth control and contraceptive services cover the full range of options available, from short-term hormonal methods to long-acting reversible contraception, so you can choose what works best for your body and lifestyle. You can also read more about how fertile you are after an abortion and whether you can get pregnant after an abortion.
Accessing Second Trimester Abortion Care
Accessing second trimester abortion care requires planning, particularly for people in states where later abortion is restricted or unavailable. Illinois is one of the most accessible states for abortion care, with strong legal protections and providers who offer care through 24 weeks and beyond in appropriate medical circumstances.
If you are traveling from another state, our guide on getting an abortion in another state covers what to expect logistically. For information on the full range of procedures available at different gestational ages, see our guide on abortion by gestational weeks.
Our in-clinic abortion services include second trimester D&E procedures performed by experienced providers in a supportive, confidential environment. For those earlier in pregnancy who may qualify, our telehealth abortion care and abortion pill services offer private, accessible options from home.
Frequently Asked Questions
Is second trimester abortion safe?
Yes. When performed by trained providers in an appropriate clinical setting, second trimester abortion is medically safe. D&E has a well-established safety record, and serious complications occur in a very small percentage of cases.
Is D&E painful?
Most people experience manageable discomfort with appropriate sedation. Cramping is the most common sensation during and after the procedure, and over-the-counter pain relievers are effective for recovery.
Can I go home the same day after a D&E?
Yes. Most patients are discharged within one to two hours of the procedure and can return home the same day.
How long does recovery take?
Most people feel physically recovered within a few days to a week. Bleeding may continue for one to two weeks. Full recovery, including the return of a normal menstrual cycle, typically occurs within four to six weeks.
Will a second trimester abortion affect future fertility?
In the vast majority of cases, a second trimester abortion does not affect future fertility. Complications that affect fertility are rare when procedures are performed by experienced providers.
What if I am past 24 weeks?
Care beyond 24 weeks is more specialized. Your provider can discuss what options exist based on your specific circumstances and gestational age.
